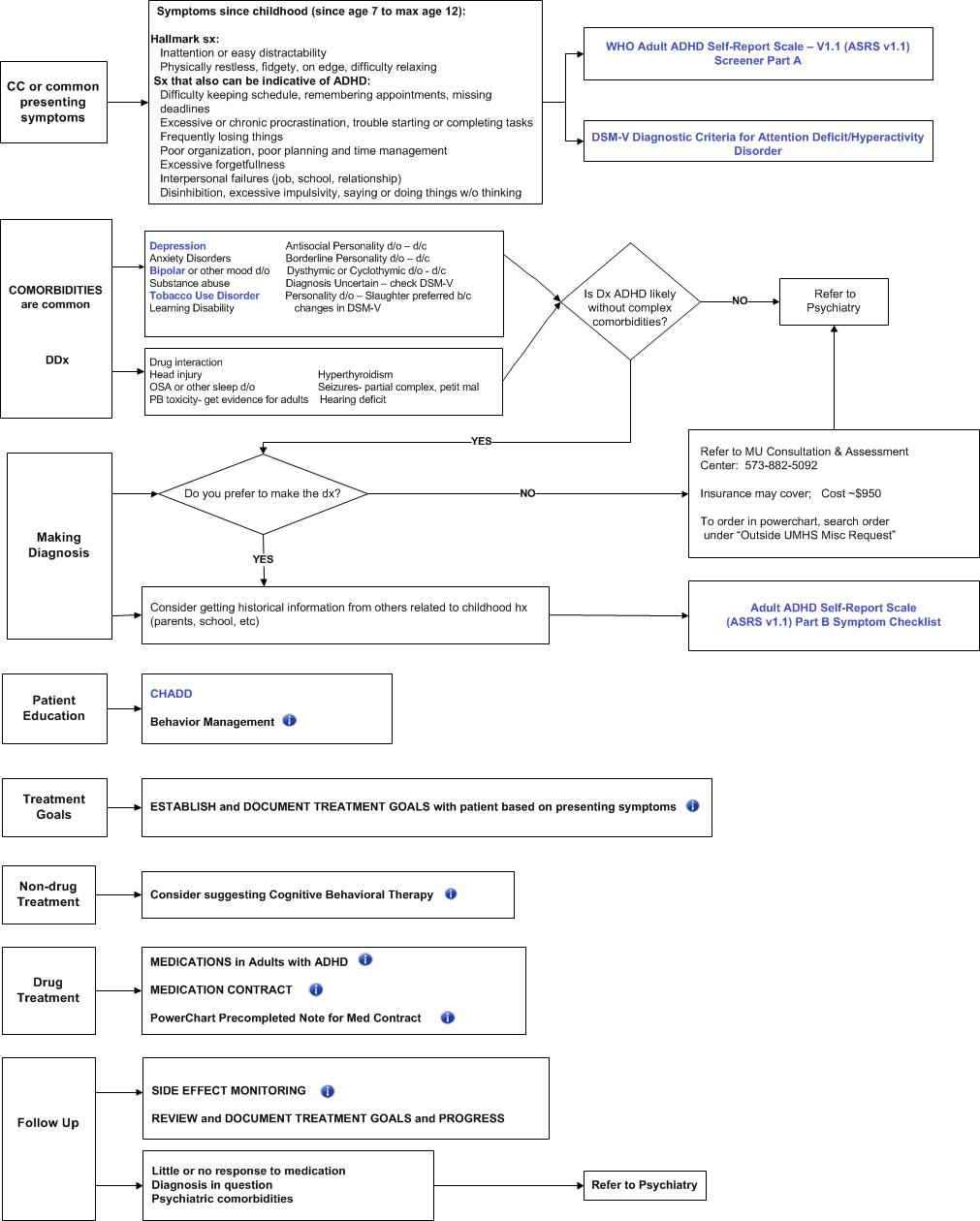
Behavior Management Ideas
Calendar, Lists
Reminder notes
Special place for keys, bills, paperwork
Break tasks into chunks
Alcohol in moderation or abstinence?
Cognitive Behavioral therapy
EXAMPLES of TREATMENT GOALS
Less distractable, able to pay attention
Less fidgety
Thinking before doing
Less procrastination
Get Written work done in reasonable time
Not losing things, less forgetful
Get organized
Finish one project before starting anotherInitiate uninteresting but necessary tasks w/o wasting time.
Family and Community Medicine ADD/ADHD MEDICATION CONTRACT
I understand and agree to the following:
I have been prescribed stimulant medication for treatment of Attention Deficit Disorder (ADD) or Attention Deficit Hyperactivity Disorder (ADHD).
ADD/ADHD stimulant medications are controlled substances that are regulated by state and federal law because of their high risk for abuse. I understand that it is a FELONY to obtain these medications by fraudulent means, to possess these medications without a legitimate prescription, and to give or sell these medications to others. I acknowledge that it is both illegal and dangerous to share or sell prescription medications.
I will be receiving written ADD/ADHD medications only from my physician listed below or their designee in the event of illness or absence. I will receive the prescription only for the time frame that my physician decides with me (either once a month or if condition is stable as deemed by the physician, once every three months).
I will use my medication as prescribed and not adjust the dosage on my own.
I am responsible for filling and paying for my medications
I will be required to make and keep regular appointment at with my physician for follow up.
I will not receive any medications earlier than they are due.
I will call in at least 3 business days to request my written refill.
Missing appointments will result in the loss of ADD/ADHD prescription privileges.
There will be no replacement of prescriptions/medications that are lost, stolen, misused or damaged and I am responsible for keeping the prescriptions or medications safe from loss, theft and/or damage.
I have read and understood this contract and I agree to fulfill my obligations and understand that any violation of this contract will results in the termination of this contract and loss of ADD/ADHD prescription given by this practice and all of the Family and Community Medicine practices in the University of Missouri-Columba
Patient Name ________________________________ Patient Signature __________________________ Date ________
Provider Name _______________________________ Provider Signature _________________________ Date ________
Sources: Marist college Health Services, Union University Health Services
Palpitations and elevated pulse rate
Appetite decline, nausea, weight changes
Sleep problems or trouble with initiation of sleep
Headache
Altered BP
Neuropsych sx: Depression, aggression, loss of creativity, flat affect, paranoia, suicidal ideation
Fatigue
SIDE EFFECTS:
STIMULANTS - inc HR, BP, cardiac arrest, arrhythmias, stroke; delayed onset of sleep, decrease appetite, wt loss, tics, abuse potential